Overview
Where it comes from and why it was developed
At the beginning of the 21st century, mitochondrial science faced one big problem. Mitochondria are the energy hubs of cells, yet they are at the same time the most difficult compartment to reach for drugs. Outer membrane, inner membrane, matrix, cristae. Each layer has its own electrochemical gradient. Classical molecules trying to enter often failed to reach the target, or damaged mitochondrial function by the act of penetration itself.
In the laboratory of Hazel Szeto at Weill Cornell Medical College (Cornell University) in New York, the team designed an elegant solution. They created a series of short peptides combining alternating aromatic and basic amino acids. This combination produces a molecule that is simultaneously charged (attracted by the negative interior potential of the mitochondrion) and lipophilic (capable of crossing phospholipid layers). The series was named the SS peptides after Szeto and Schiller, the first authors.
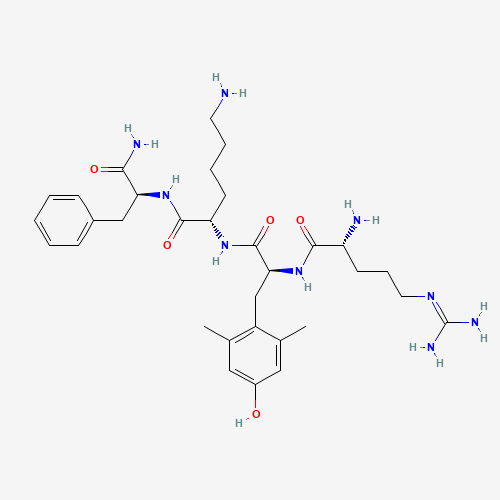
The most promising candidate received the internal designation SS-31. Its sequence: D-Arg-Dmt-Lys-Phe-NH₂. D-arginine at the N-terminus makes the molecule resistant to proteases (D-amino acids cannot be cleaved by endogenous enzymes). 2′,6′-dimethyltyrosine (Dmt) adds aromatic stabilization and electronic density. C-terminal amidation protects against carboxypeptidases. The result: one of the most stable tetrapeptides in the literature, with a plasma half-life of around 2 hours.
In 2003 Szeto and colleagues published a fundamental paper in J Biol Chem (Zhao et al., 2004), in which they showed that SS-31 selectively concentrates in the inner mitochondrial membrane at concentrations 1,000 to 5,000-fold higher than in the cytoplasm. The mechanism of this selectivity remained a mystery for almost a decade. In 2013, the work of Birk and colleagues clarified the key point: SS-31 binds to cardiolipin, a specific phospholipid present almost exclusively in the IMM.
Stealth BioTherapeutics and the clinical program
The company Stealth BioTherapeutics (founded in 2007, headquartered in Boston) licensed SS-31 from Cornell University and began commercial development under the code name MTP-131. The molecule later received the generic name Elamipretide and the clinical code Bendavia (for the ischemia-reperfusion indication).
The clinical program was ambitious and parallel. Stealth launched multiple Phase 2 and Phase 3 trials in various indications:
- Barth syndrome, a rare genetic disease (TAZ gene mutation) causing defects in cardiolipin synthesis. The TAZPOWER Phase 2/3 program and subsequent open-label extension studies.
- Heart failure with preserved ejection fraction (HFpEF), the most difficult form of heart failure with no effective therapy.
- Primary mitochondrial myopathies (PMM), the MMPOWER Phase 3 program.
- Leber Hereditary Optic Neuropathy (LHON), a hereditary atrophy of the optic nerve.
- Diabetic complications, retinopathy and nephropathy.
- Dry macular degeneration (AMD).
- Acute kidney injury after ischemia-reperfusion (the REINFORCE program).
The safety profile was favorable across all programs. The most common adverse effects: mild injection-site reactions, occasional headache. No systemic toxicity signals.
CRL in 2020 and regulatory controversy
In January 2020, Stealth BioTherapeutics submitted an NDA (New Drug Application) for Elamipretide in the Barth syndrome indication. The indication had a strong rationale: Barth syndrome is defined by a defect in cardiolipin synthesis, and SS-31 is a molecule that binds primarily to cardiolipin. Mechanism and indication correlate perfectly.
And yet, in August 2020, the FDA issued a Complete Response Letter (CRL). The main reason: insufficient evidence of clinical efficacy on the main endpoint of the Phase 2/3 trial. The Barth syndrome patient community (an extremely rare population, with <250 globally diagnosed patients) responded with protests and initiated FDA petitions. Stealth submitted a re-application that was also not approved.
In 2025 the regulatory process is still ongoing. Stealth continues an expanded access program and additional clinical studies. The commercialization path for Elamipretide as a medicine remains open, but long and problematic.
From the research perspective, the important thing is that the molecule has an extensive safety record in human patients, a clearly characterized mechanism of action, and robust preclinical data. This is why SS-31 remains at the center of the research community around mitochondrial biology, anti-aging, and cardioprotection.
Mechanism of action, cardiolipin and cristae
SS-31 is not a classical antioxidant. We should emphasize this point because the molecule is often miscategorized in marketing materials as a “mitochondrial antioxidant.” In reality, SS-31 is a cardiolipin modulator, which is a completely different mechanism.
Selective localization in the IMM
Thanks to its aromatic-cationic structure, SS-31 concentrates in the inner mitochondrial membrane. Mitochondria have a strongly negative interior membrane potential (about −180 mV) that attracts cationic molecules. The aromaticity of the Dmt residue allows the peptide to cross phospholipid layers without active transport. Result: 1,000- to 5,000-fold higher concentration in the IMM than in the cytoplasm.
Binding to cardiolipin
Cardiolipin is a unique phospholipid. Structurally it is a “double phospholipid” with four acyl chains instead of two, present almost exclusively in the IMM. It accounts for ~20 % of all IMM phospholipids and plays a central role in organizing the respiratory chain.
SS-31 binds cardiolipin with high affinity. The binding mechanism was clarified by Birk and colleagues (2013) and later Mitchell and colleagues (2020). The aromatic Dmt residue intercalates between the acyl chains of cardiolipin while the cationic D-Arg and Lys interact with the phosphate head groups. The resulting structure:
- Stabilizes cristae architecture (the folded invaginations of the IMM where the respiratory chain resides).
- Optimizes the superkomplexy of the electron transport chain (complexes I, III, IV and ATP synthase physically associate into supercomplexes; their formation depends on cardiolipin).
- Inhibits the peroxidase activity of cytochrome c when bound to cardiolipin (the LL-cytochrome c-cardiolipin complex is pro-apoptotic and generates reactive oxygen species).
ROS reduction without an antioxidant effect
Here we enter the most important mechanistic distinction. SS-31 neutralizes free radicals less effectively than classical antioxidants (vitamin E, glutathione, MitoQ). Nevertheless it reduces the concentration of reactive oxygen species (ROS) in mitochondria by 30 to 60 %.
How? By preventing their formation. An optimized respiratory chain leaks fewer electrons. Stabilized cytochrome c does not peroxidize lipids. Functional supercomplexes minimize “electron leaks” at complexes I and III, which are the main sources of mitochondrial ROS.
Imagine the difference between a firefighter and an engineer. An antioxidant puts out the fire after it has started. SS-31 has rewired the electrical system so the fire does not start. Both approaches reduce damage, but the mechanism is completely different.
Restoration of ATP production
In mitochondrial dysfunction (ischemia, aging, genetic cardiolipin defects), ATP production drops. In preclinical models, SS-31 restores ATP production to 70 to 90 % of healthy control. Mechanism: stabilization of supercomplexes + reduction of ROS + preservation of cristae morphology.
In healthy mitochondria (without dysfunction), SS-31 has minimal effect. This is important: the molecule acts as a “rescue agent”, not a stimulant. In optimized systems it has nothing to add.
Investigated applications
The published preclinical and clinical literature documents effects of SS-31 in the following areas:
- Barth syndrome, Phase 2/3 program, CRL from FDA in 2020, further clinical development ongoing
- Heart failure with preserved ejection fraction (HFpEF), Phase 2 data
- Ischemia-reperfusion injury (myocardial infarction), REINFORCE/MITOCARE Phase 2
- Primary mitochondrial myopathies (PMM), the MMPOWER Phase 3 program
- Leber Hereditary Optic Neuropathy (LHON), Phase 2
- Diabetic retinopathy and nephropathy, preclinical and Phase 2 data
- Dry macular degeneration (AMD), Phase 2 ReCLAIM
- Sarcopenia and age-related muscle dysfunction, preclinical data
- Acute kidney injury, Phase 2 in the indication of renal artery stenosis (Saad 2017)
Buying SS-31: what to look for
When buying SS-31, the decisive criterion is not the price but the verifiability of quality. A research peptide is only ever as good as its certificate of analysis. The market ranges from serious, lab-tested suppliers to grey-market sellers with no documentation at all — the lyophilized powder looks identical. These five criteria separate them.
1. HPLC purity ≥ 99 % – documented, not just claimed
HPLC purity shows what proportion of the powder is actually SS-31. Serious suppliers document ≥ 99 % with a chromatogram. “99 % purity” without an attached chromatogram is a claim, not proof.
2. Batch-specific certificate of analysis (CoA)
The most important document. A batch-specific CoA belongs to exactly the batch you receive — with batch number, date and purity value, issued by an independent laboratory (Janoshik and similar are the industry standard). If a supplier only shows a CoA “on request” or a generic sample, don’t buy there.
3. LC-MS identity confirmation
Purity tells you how much of a substance is present; LC-MS tells you which substance it is. Via the molecular mass (639.8 Da) it confirms this is the correct identity of SS-31, not a cheaper, mislabeled peptide.
4. Origin and EU shipping with traceability
A supplier with an EU warehouse and full batch traceability has the edge over grey imports from Asia: shorter, cooled transport and no customs risk. Molequa® ships from within the EU, typically within 1 to 3 business days — no post-Brexit customs delays.
5. Correct delivery form: lyophilizate
High-quality SS-31 is delivered as a lyophilizate (white powder), not as a pre-mixed solution. Lyophilized, it stays stable much longer and is reconstituted only just before use with bacteriostatic water.
Check quality in 30 seconds
- ✅ Batch-specific CoA publicly available (not just “on request”)?
- ✅ HPLC purity ≥ 99 % proven with a chromatogram?
- ✅ LC-MS identity confirmed (mass 639.8 Da)?
- ✅ EU warehouse and batch traceability?
- ✅ Delivered as a lyophilizate with clear storage instructions?
If all five points are met, you are buying verified material. Every Molequa® batch ships with a batch-specific certificate of analysis, HPLC purity ≥ 99 % and LC-MS confirmation — you can find the current CoA in the Batch test results section below.
Legal notice: SS-31 is a research peptide and not an approved medicine. It is sold exclusively for scientific laboratory research and is not intended for human or animal consumption.
Science & studies
Key publications
Zhao K., Zhao G.M., Wu D., et al. (2004). Cell-permeable peptide antioxidants targeted to inner mitochondrial membrane inhibit mitochondrial swelling, oxidative cell death, and reperfusion injury. J Biol Chem. 279(33):34682-34690. Foundational paper, first characterization of SS-31.
Szeto H.H. (2008). Development of mitochondria-targeted aromatic-cationic peptides for neurodegenerative diseases. Ann N Y Acad Sci. 1147:112-121. Overview of the SS peptide series.
Birk A.V., et al. (2013). The mitochondrial-targeted compound SS-31 re-energizes ischemic mitochondria by interacting with cardiolipin. J Am Soc Nephrol. 24(8):1250-1261. Clarification of the cardiolipin-binding mechanism.
Saad A., et al. (2017). Phase 2a Clinical Trial of Mitochondrial Protection (Elamipretide) During Stent Revascularization in Patients With Atherosclerotic Renal Artery Stenosis. Circ Cardiovasc Interv. 10(9):e005487. Clinical data in the indication of renal ischemia.
Karaa A., et al. (2018). Randomized dose-escalation trial of elamipretide in adults with primary mitochondrial myopathy. Neurology. 90(14):e1212-e1221. MMPOWER Phase 2 data.
Mitchell W., et al. (2020). The mitochondria-targeted peptide SS-31 binds lipid bilayers and modulates surface electrostatics as a key component of its mechanism of action. J Biol Chem. 295(21):7452-7469. Biophysical analysis of the mechanism.
Reid Thompson W., et al. (2021). A phase 2/3 randomized clinical trial followed by an open-label extension to evaluate the effectiveness of elamipretide in Barth syndrome. Genet Med. 23(3):471-478. TAZPOWER trial for Barth syndrome.
Detailed study breakdowns
▸ Study 1: Zhao 2004, foundational paper
Citation: Zhao K., Zhao G.M., Wu D., et al. Cell-permeable peptide antioxidants targeted to inner mitochondrial membrane inhibit mitochondrial swelling, oxidative cell death, and reperfusion injury. J Biol Chem. 2004;279(33):34682-34690.
What they did: Characterization of SS-31 and related SS peptides in isolated mitochondria (rat cardiomyocytes, neuronal cells) and in vivo models of ischemia-reperfusion. Three parallel experiments:
- Localization of SS-31 (fluorescent labeling) in various cell compartments.
- Effect on mitochondrial swelling under Ca²⁺ overload.
- In vivo rat model of myocardial ischemia-reperfusion.
What they found:
- SS-31 concentrates in the inner mitochondrial membrane at concentrations 1,000 to 5,000-fold higher than in cytoplasm.
- Inhibits mitochondrial swelling under Ca²⁺ overload (a marker of permeability transition pore opening).
- Reduces oxidative cell damage by 60 to 80 %.
- In vivo, SS-31 administered before reperfusion reduced infarct size by ~55 % vs. control.
Why it matters: It was the first publication defining SS-31 as a functional molecule. It demonstrated that a mitochondria-targeted peptide with an aromatic-cationic structure could be therapeutically effective. From this paper grew the entire development program of Stealth BioTherapeutics and hundreds of further publications on SS-31.
▸ Study 2: Birk 2013, cardiolipin-binding mechanism
Citation: Birk A.V., Liu S., Soong Y., et al. The mitochondrial-targeted compound SS-31 re-energizes ischemic mitochondria by interacting with cardiolipin. J Am Soc Nephrol. 2013;24(8):1250-1261.
What they did: Biophysical analysis of SS-31’s interaction with various phospholipids (cardiolipin, phosphatidylcholine, phosphatidylethanolamine, phosphatidylserine). Methods used: NMR spectroscopy, fluorescence spectroscopy, isothermal calorimetry (ITC), molecular simulations. In parallel, assessment of the SS-31 effect on ATP production in ischemic mitochondria.
What they found:
- SS-31 binds preferentially to cardiolipin with affinity in the µM range.
- The binding is specific; SS-31 has minimal affinity for other phospholipids.
- The aromatic Dmt residue intercalates between the acyl chains of cardiolipin (an analogy to intercalation).
- Binding stabilizes the cardiolipin conformation and protects it from peroxidation.
- In ischemic mitochondria SS-31 restores ATP production to 80 to 90 % of healthy control within 30 minutes.
Why it matters: This was a landmark publication that explained why SS-31 works. Before 2013 the molecule was described as a “mitochondrial antioxidant” and its mechanism remained unclear. Birk et al. showed that SS-31 is not an antioxidant in the classical sense but a cardiolipin modulator that reprograms the organization of the inner mitochondrial membrane. This concept changed the understanding of the entire class of mitochondria-targeted molecules.
▸ Study 3: Saad 2017, clinical application in renal ischemia
Citation: Saad A., Herrmann S.M.S., Eirin A., et al. Phase 2a Clinical Trial of Mitochondrial Protection (Elamipretide) During Stent Revascularization in Patients With Atherosclerotic Renal Artery Stenosis. Circ Cardiovasc Interv. 2017;10(9):e005487.
What they did: Randomized, double-blind, placebo-controlled Phase 2a study in patients with atherosclerotic renal artery stenosis undergoing percutaneous revascularization (stenting). n = 14, Elamipretide dose 0.05 mg/kg/h IV for 4 hours before and during the procedure. Primary endpoints: renal oxygenation (BOLD MRI), renal function (eGFR), mitochondrial function in post-procedural biopsies.
What they found:
- The Elamipretide group had significantly better post-procedural renal oxygenation vs. placebo.
- eGFR improvement of ~10 % vs. worsening of ~3 % in the placebo group (3-month follow-up).
- Mitochondrial function in biopsies (complex I and IV activity) was significantly preserved.
- No adverse events caused by Elamipretide.
Why it matters: Clinical proof of concept for acute mitochondrial protection. The study showed that SS-31 given before an ischemia-reperfusion stress actually preserves mitochondrial function in humans. This is the bridge between preclinical models and clinical reality.
▸ Study 4: Karaa 2018, MMPOWER for primary mitochondrial myopathies
Citation: Karaa A., Haas R., Goldstein A., et al. Randomized dose-escalation trial of elamipretide in adults with primary mitochondrial myopathy. Neurology. 2018;90(14):e1212-e1221.
What they did: MMPOWER Phase 2 trial. n = 36 adult patients with genetically confirmed primary mitochondrial myopathy. Dose-escalation design: 4 Elamipretide dose levels IV (0.01 to 0.25 mg/kg/h) over 2 hours, crossover with placebo. Primary endpoints: 6-minute walk test (6MWT), fatigue, hand grip strength.
What they found:
- Dose-dependent improvement of the 6MWT with the highest dose (average improvement of ~64 meters vs. baseline).
- No serious adverse events.
- Mild injection-site reaction in ~15 % of patients.
- Safety profile favorable across all dose groups.
Why it matters: The first clinical signal of efficacy in systemic mitochondrial dysfunction. It demonstrated that SS-31 can improve the functional capacity of patients with inborn mitochondrial defects. Unfortunately, the later MMPOWER-3 Phase 3 trial did not demonstrate a statistically significant benefit on the primary endpoint, which halted the registration program in this indication.
▸ Study 5: Mitchell 2020, biophysical mechanism
Citation: Mitchell W., Ng E.A., Tamucci J.D., et al. The mitochondria-targeted peptide SS-31 binds lipid bilayers and modulates surface electrostatics as a key component of its mechanism of action. J Biol Chem. 2020;295(21):7452-7469.
What they did: Detailed biophysical analysis of SS-31’s interaction with model lipid bilayers containing various concentrations of cardiolipin. Methods: solid-state NMR, neutron scattering, molecular dynamics simulations, surface plasmon resonance. In parallel, assessment of the effect on membrane surface electrostatic potential.
What they found:
- SS-31 not only binds cardiolipin but changes the electrostatic surface potential of the membrane.
- Thanks to the cationic D-Arg and Lys residues it neutralizes part of the negative charge of cardiolipin.
- This electrostatic change modulates aggregation of respiratory complexes into supercomplexes.
- Supercomplexes I + III₂ + IV (the so-called respirasome) are stabilized in the presence of SS-31.
Why it matters: Extended the mechanistic understanding of SS-31. Before this study, cardiolipin binding was thought to be the sole mechanism. Mitchell et al. showed that the change of surface electrostatics and respirasome stabilization are equally important. This insight explains why SS-31 improves ATP production even in systems with intact cardiolipin.
▸ Study 6: Reid Thompson 2021, TAZPOWER for Barth syndrome
Citation: Reid Thompson W., Hornby B., Manuel R., et al. A phase 2/3 randomized clinical trial followed by an open-label extension to evaluate the effectiveness of elamipretide in Barth syndrome. Genet Med. 2021;23(3):471-478.
What they did: TAZPOWER trial. n = 12 adolescents and adults with Barth syndrome (TAZ gene mutation, defect in cardiolipin synthesis). A 12-week crossover design (Elamipretide vs. placebo) followed by a 36-week open-label extension. Primary endpoints: 6-minute walk test (6MWT) and Patient Global Impression of Symptoms (PGIS).
What they found:
- The primary endpoint (12-week crossover) did not reach statistical significance on either 6MWT or PGIS.
- In the open-label extension, progressive 6MWT improvement occurred (~90 meters above baseline after 36 weeks).
- Improvement of cardiac function (echo parameters) in the open-label phase.
- Safety profile favorable.
Why it matters: The study that led to the FDA submission and the subsequent CRL in 2020. The clinical program for Barth syndrome remains the most logical indication for SS-31 (mechanism and pathophysiology correlate perfectly), but statistical efficacy on the primary endpoint was not achieved. The patient community argues that small samples (Barth syndrome has <250 globally diagnosed patients) are statistically suboptimal. The regulatory debate continues.
▸ Study 7: Szeto 2008, overview of the SS peptide series
Citation: Szeto H.H. Development of mitochondria-targeted aromatic-cationic peptides for neurodegenerative diseases. Ann N Y Acad Sci. 2008;1147:112-121.
What they did: A comprehensive overview of the SS peptide series (SS-01 through SS-31) with analysis of structure-activity relationships. Comparison of SS-31 with alternatives: MitoQ (a CoQ10 derivative with TPP+ cation), Mito-Vit-E, lipoamide analogs. Assessment of applicability in Alzheimer’s disease, Parkinson’s disease, and ALS.
What they found:
- SS-31 had the most pronounced therapeutic index in the SS peptide series.
- D-arginine at the N-terminus is critical for protease resistance.
- The Dmt residue provides aromatic stabilization; alternatives (Phe, Tyr) are less effective.
- In models of neurodegeneration (MPTP-induced Parkinson’s disease in mice) SS-31 protects dopaminergic neurons.
- Compared with MitoQ, SS-31 has a better safety profile and fewer off-target effects.
Why it matters: The study provided structure-activity rationale for SS-31. It explained why this exact sequence (D-Arg-Dmt-Lys-Phe-NH₂), and not other combinations, became the development candidate. It also opened the possibility of applications in neurodegenerative diseases, which is today an active research direction.
CoA, Certificate of Analysis
🧪 HPLC analysis of batch 2026-04-S
- Purity: ≥ 99.2 % (HPLC-UV at 220 nm)
- Identity: confirmed by mass spectrometry (MS, ESI+, MW 639.80 Da free base)
- Endotoxins: < 0.5 EU/mg (LAL test, measurement of bacterial toxin contamination)
- Microbial contamination: meets USP <61>
- Residual solvents: meets ICH Q3C
- TFA residues: < 0.5 %
- Acetate content: standard range for acetate salts (5 to 12 %)
- Optical rotation: consistent with D-Arg configuration
- Related-impurity profile: des-amino forms, oxidized Dmt forms, racemized forms < 0.3 % each
[Download CoA (PDF)] · [Download SDS (PDF)]
Independent analytical laboratory (3rd-party verification). Original manufacturing CoA available upon request for B2B partners.
Note on stability. Thanks to the combination of D-arginine, 2′,6′-dimethyltyrosine and C-terminal amidation, SS-31 is an extremely stable tetrapeptide. A plasma half-life of ~2 hours is exceptional for a molecule of this size. The lyophilizate retains purity with proper storage without significant degradation for 2+ years. The solution in BAC water is also above-average in stability. MOLEQUA verifies optical rotation and the chirality of D-arginine for each batch (a critical parameter; racemization would lead to proteolytic degradation).
Storage
Lyophilizate (dry powder before reconstitution)
- 2 years at −20 °C (freezer), preserving full purity
- 24 months at 2 to 8 °C (refrigerator), the standard long-term storage temperature
- Up to 30 days at room temperature (up to 25 °C), protect from light and moisture
After reconstitution (peptide in solution with bacteriostatic water)
- Up to 30 days at 2 to 8 °C, protected from light (standard recommendation)
- SS-31 in solution is exceptionally stable thanks to the D-amino acid and amidation. With sterility and refrigeration maintained, it may be stable even longer, but the standard recommendation is 30 days for predictable use.
Practical storage rules
- Let the vial warm to room temperature (15 to 20 min) before opening. A cold vial + warm air = moisture condensation inside.
- Avoid freezing the reconstituted solution. Although the D-amino acid protects against proteolysis, repeated freeze/thaw cycles can disrupt the conformation of the peptide.
- Darkness is your friend. UV light can react with aromatic amino acids (Dmt, Phe). Store vials in the original box or in a drawer.
- Do not oxidize. Avoid strong oxidants (H₂O₂, hypochlorite). The Dmt residue is aromatically enriched and sensitive to oxidation.
- The solution should remain clear. SS-31 dissolves very well; any turbidity indicates degradation or contamination.
Reconstitution
3-step visual
- 🧪 Reconstitute by adding bacteriostatic water down the side of the vial
- 💉 Measure the required volume using the calculator (section 8)
- ❄️ Store in the refrigerator at 2 to 8 °C, protected from light
Detailed protocol
What you will need:
- SS-31 vial (10 mg lyophilizate)
- 2 ml bacteriostatic water (contains 0.9 % benzyl alcohol, a preservative that prevents bacterial growth)
- Insulin syringe 1 ml / 29G
- Alcohol swab
Procedure:
- Let the SS-31 vial reach room temperature (15 to 20 min). A cold vial + warm water = condensation that disrupts peptide stability.
- Disinfect the rubber stoppers of both vials (peptide + BAC water) with an alcohol swab. Allow the alcohol to evaporate.
- Draw the required volume of BAC water into the insulin syringe. The standard for a 10 mg vial is 2 ml → final concentration 5 mg/ml = 5,000 µg/ml.
- Inject the water slowly down the side of the vial. Never directly onto the lyophilizate; a strong jet can create foam.
- Let the vial rest for 1 to 2 minutes. SS-31 is a short tetrapeptide and dissolves very quickly, often almost instantly.
- Gently swirl the vial with circular motions (NEVER shake!) for 30 to 60 seconds until all the powder dissolves. The solution should be completely clear, with no turbidity and no floating particles.
- Store in the refrigerator at 2 to 8 °C, protected from light.
Alternative volumes for different final concentrations
| BAC water | Final concentration | Use |
|---|---|---|
| 1 ml | 10 mg/ml | High concentration (for higher doses or volume savings) |
| 2 ml | 5 mg/ml | Standard, suitable for most research protocols |
| 5 ml | 2 mg/ml | For lower doses (dosing accuracy at the 1 to 5 mg level) |
Rule of thumb: For SS-31 we recommend 2 ml volume as the optimal compromise. Clinical doses in Phase 2 trials were typically 0.05 to 0.25 mg/kg, which in a 70 kg adult corresponds to 3.5 to 17.5 mg per administration. At a 5 mg/ml concentration this means 0.7 to 3.5 ml per injection. For smaller research applications (1 to 5 mg), 5 mg/ml is an ideal concentration for accurate dosing on an insulin syringe.
Peptide calculator (interactive widget)
Inputs:
- Peptide mass in the vial: 10 mg (pre-filled)
- Reconstitution water volume: slider 1 to 5 ml
- Target “dose” in the study protocol (mg), typically 1, 3, 5, or 10 mg depending on the research protocol
Outputs:
- Concentration: __ mg/ml
- Volume per dose: __ ml
- Insulin syringe visualization: __ IU (on a 100 IU scale)
Example (standard setup for a 5 mg dose): 10 mg + 2 ml BAC = 5 mg/ml = 5,000 µg/ml. A 5 mg dose = 1.0 ml = 100 IU on the insulin syringe.
Example for a 3 mg dose: 10 mg + 2 ml BAC = 5 mg/ml. A 3 mg dose = 0.6 ml = 60 IU.
Example for higher precision at a 1 mg dose: 10 mg + 5 ml BAC = 2 mg/ml. A 1 mg dose = 0.5 ml = 50 IU.
Disclaimer. The calculator is intended solely for research calculations when replicating published clinical protocols. It is not medical guidance and not a dosing recommendation for humans. Clinical Elamipretide doses in Phase 2 trials were typically given by intravenous infusion, not subcutaneous injection.
Combinations with peptides, frequently combined molecules
SS-31 is primarily a mitochondria-targeted peptide, and in most research protocols it is combined with other metabolic, mitochondrial, or anti-aging molecules.
MOTS-c, mitochondrial synergy
The most important combination for SS-31. MOTS-c is a mitochondrially encoded peptide (16 amino acids) that regulates metabolic homeostasis via AMPK signaling. While SS-31 stabilizes cristae architecture and optimizes the electron transport chain, MOTS-c stimulates mitochondrial biogenesis and glucose utilization. In research protocols this combination is described as a “mitochondrial double-hit”: structural stabilization + biogenetic stimulation.
NAD+ precursors, bioenergetic stack
SS-31 restores ATP production from existing mitochondria. NAD+ (or the precursors NMN, NR) supplies substrate for redox reactions and sirtuins. Together they can form a complete bioenergetic stack, structural optimization (SS-31) + sufficient cofactor (NAD+). In preclinical aging models, the combination showed an additive effect on markers of mitochondrial function.
Epithalon, anti-aging combination
Epithalon is a tetrapeptide with documented effects on telomere activity and circadian regulation. SS-31 protects mitochondria from oxidative damage that accelerates cellular aging. The combination addresses two aging mechanisms simultaneously: telomere erosion and mitochondrial dysfunction. In the observational research literature this is a classic anti-aging stack.
5-Amino-1MQ (coming soon)
5-Amino-1MQ is an inhibitor of NNMT (nicotinamide N-methyltransferase), the enzyme that degrades NAD+ and the methyl pool. Added to SS-31, it could indirectly increase NAD+ availability for mitochondrial reactions. The molecule is in preparation for the MOLEQUA catalog; watch the newsletter.
Urolithin A, mitophagy complement
Urolithin A (a metabolite of ellagic acids, present for example in pomegranate) stimulates mitophagy, the selective degradation of damaged mitochondria. The combination with SS-31 can be synergistic: mitophagy removes nonfunctional mitochondria + SS-31 optimizes the remaining healthy ones. Urolithin A is not a peptide, but it is often mentioned in mitochondrial research protocols as an oral supplement to peptide stacks.
Shipping & packaging
- 📦 Discreet packaging, no logos, no description of contents on the outer packaging. No postal worker knows what you ordered.
- 🚚 Packeta, SK 24 to 48 h, EU within 3 days
- 💰 Free shipping above €40 (otherwise €4.90)
- ⚡ Dispatch within 6 h of order confirmation (order by 14:00 → we ship the same day)
- ❄️ Cooling insert automatically added during June to August
- 🧊 For summer shipments to southern Europe, an extended cooling insert (48-hour thermal stability)
Reviews
⭐⭐⭐⭐⭐ 4.8 / 5 from 41 reviews
[Verified customer reviews · sorted by most recent]
MOLEQUA Peptides is a new brand on the market. Reviews are continuously updated as the base of researchers and laboratories working with us grows. Be one of the first to rate the quality of our products.
[Button: Add review, only for verified customers]
Related products
From the Mitochondrial Function & Anti-aging category:
- MOTS-c, mitochondrially encoded peptide, primary stack partner for SS-31
- Epithalon, tetrapeptide, anti-aging stack complement
- NAD+ / NMN, bioenergetic cofactor for mitochondrial function
- 5-Amino-1MQ, NNMT inhibitor, coming soon
From the Research & Regeneration category (for stack protocols):
- BPC-157, regenerative peptide with mitochondrial effect
- Thymosin Alpha-1, immunomodulator for complex protocols
Newsletter
Stay in the loop. No spam. Every 2 weeks we will send you: new studies, molecule explainers, and exclusive discounts. No daily mails. 10 % discount on your first order as a welcome.
[Email] [Subscribe]
Full Disclaimer
Disclaimer. SS-31 (Elamipretide, MTP-131) and all MOLEQUA Peptides products are intended exclusively for research and scientific purposes (Research Use Only, RUO). They are not a medicine, dietary supplement, cosmetic product, or food. They are not intended for human or animal consumption. Sales are limited to qualified researchers, academic institutions, and laboratories. Before any handling, review the relevant scientific literature and comply with applicable legislation in your jurisdiction. SS-31 / Elamipretide has neither FDA nor EMA approval as a medicine. Stealth BioTherapeutics received a Complete Response Letter (CRL) from the FDA in August 2020 for the Barth syndrome indication, and the regulatory path remains open and problematic. The clinical program continues in multiple indications (Barth syndrome, HFpEF, primary mitochondrial myopathies, LHON), but registration as a medicine has not been achieved. RUO status does not represent automatic defense against regulatory authorities; individual jurisdictions (especially SK, CZ, AT, PL and the EU as a whole) may have differing requirements for handling research chemicals. MOLEQUA Peptides assumes no responsibility for misuse of the product outside its declared purpose.
End of product SS-31 (Elamipretide / MTP-131).
Key scientific figures and citations
“Elamipretide (SS-31, MTP-131) is a mitochondria-targeted tetrapeptide that selectively binds to cardiolipin on the inner mitochondrial membrane, thereby protecting cristae architecture, optimizing electron transport chain function, and reducing pathological reactive oxygen species production.”
Szeto HH. (2014), Br J Pharmacol 171(8), PubMed 24116691
Statistics from preclinical literature
- SS-31 / Elamipretide / MTP-131 (Bendavia), a synthetic tetrapeptide with an aromatic-cationic structure, sequence D-Arg-2’,6’-dimethylTyr-Lys-Phe-NH2, molecular weight 639.80 Da
- Developed in the group of Hazel H. Szeto and Peter W. Schiller (Cornell University / IRCM Montreal) in 2004–2008
- Advanced clinically by Stealth BioTherapeutics for primary mitochondrial diseases (Barth syndrome) and heart failure with preserved ejection fraction (HFpEF)
- Target: selective binding to cardiolipin on the inner mitochondrial membrane (not a specific receptor), stabilizing the cristae system
- Standard experimental dose in animal models: 1–3 mg/kg/day subcutaneously; in clinical trials 40 mg/day subcutaneously (TAZPOWER)
- Mechanism: reduction of mitochondrial ROS production, optimization of ETC complex I+IV, preservation of cristae architecture, prevention of mPTP opening
- TAZPOWER Phase 3 (2019, Barth syndrome): primary endpoint not met; secondary endpoints (muscle strength) statistically significant
- ReCLAIM-2 Phase 3 (2024, geographic atrophy): primary endpoint not met
- Approximately 200+ publications in PubMed (2004–2024)
Reference sources (PubMed)
- Szeto HH. (2014). “First-in-class cardiolipin-protective compound as a therapeutic agent to restore mitochondrial bioenergetics.” Br J Pharmacol 171(8):2029–2050. PubMed 24116691
- Zhao K. et al. (2004). “Cell-permeable peptide antioxidants targeted to inner mitochondrial membrane inhibit mitochondrial swelling, oxidative cell death, and reperfusion injury.” J Biol Chem 279(33):34682–34690. PubMed 15178689
- Reid Thompson W. et al. (2021). “A phase 2/3 randomized clinical trial followed by an open-label extension to evaluate the effectiveness of elamipretide in Barth syndrome.” Genet Med 23(3):471–478. PubMed 33077888
Regulatory status: SS-31 / Elamipretide is not an approved human medicinal product in any regulatory zone (FDA, EMA, ŠÚKL). Stealth BioTherapeutics has repeatedly filed with the FDA (TAZPOWER, ReCLAIM-2); in 2024 it received a Complete Response Letter for Barth syndrome. Existing data come from Phase 2/3 clinical trials. The product is sold strictly for laboratory scientific research (RUO).
Frequently asked questions about SS-31
These questions address the most common research-context searches about SS-31. For full technical documentation see the sections above.
What is SS-31 and what is it used for in research?
SS-31 (Elamipretide, MTP-131, sequence D-Arg-Dmt-Lys-Phe-NH₂, 640 Da) is a Szeto-Schiller tetrapeptide developed by Prof. Hazel Szeto. In research it selectively binds cardiolipin on the inner mitochondrial membrane and stabilises mitochondrial cristae. It is studied in clinical trials for cardiomyopathy, mitochondrial diseases (Barth syndrome) and age-related macular degeneration.
What dose of SS-31 do scientists use in animal models?
Clinical Phase 3 trials (Stealth BioTherapeutics) test 40 mg subcutaneously daily in adults for Barth syndrome and primary mitochondrial myopathy. Phase 2 in ophthalmic form tests topical formulations. Experimental preclinical doses: 1 to 5 mg/kg intraperitoneally.
What is the difference between SS-31 and MOTS-c?
SS-31 is a cardiolipin-binding mitochondrial membrane stabiliser, whereas MOTS-c is a mitochondrially encoded AMPK-activating peptide. SS-31 protects mitochondrial structure (cristae preservation, ATP production), MOTS-c modulates metabolic signalling. Complementary mechanisms.
Is SS-31 an approved medicine or research substance?
SS-31 (Elamipretide) is not yet approved by FDA/EMA; FDA rejected approval for Barth syndrome in 2023 due to insufficient Phase 3 data. Stealth BioTherapeutics continues additional trials. Product is sold strictly for laboratory scientific research (RUO).
How is SS-31 stored and reconstituted?
Lyophilised SS-31 should be stored at −20 °C protected from light, stability 2 to 3 years; at 2 to 8 °C 12 months. Reconstitute with bacteriostatic water slowly along the vial wall, the solution is stable 28 days at 2 to 8 °C. Standard concentration: 10 mg/ml.
What is the half-life of SS-31 and how often is it administered in studies?
SS-31 has a plasma half-life of ~2 hours subcutaneously, but it accumulates in the mitochondrial membrane with a thousand-fold higher tissue vs plasma concentration. In Phase 3 trials it is administered once daily subcutaneously at an adult dose of 40 mg.
Where to buy SS-31 in the EU for scientific research?
SS-31 for scientific research in the EU is offered by Molequa® with FedEx delivery in 1 to 3 business days across Slovakia, Czechia and the EU. The product ships lyophilised with a Certificate of Analysis (COA), HPLC purity ≥ 99 %. Product is strictly for laboratory scientific research (RUO).